
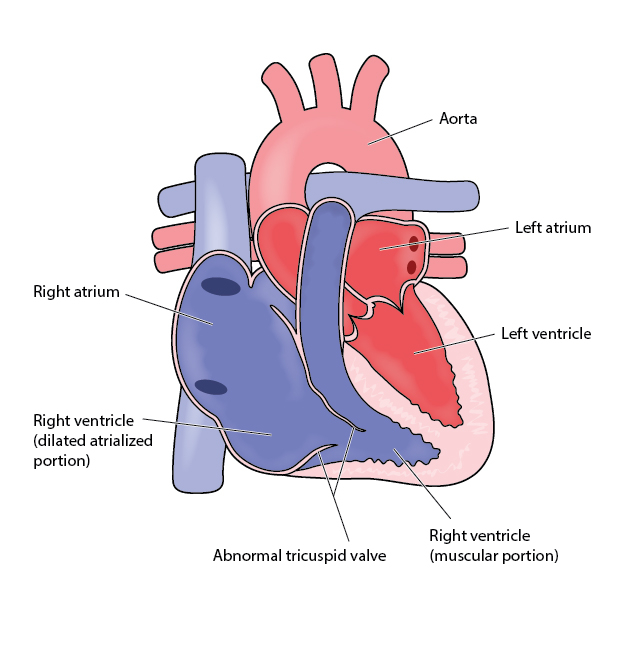
 This is a cyanotic congenital heart disease. In this anomaly,septal and posterior leaflets of tricuspid valve are not normally located and positioned much below the true location. Sometimes, it can be seen as critical congenital heart defect in newborn period, in which neonates are very sick and may die if no active treatment started early.
This is a cyanotic congenital heart disease. In this anomaly,septal and posterior leaflets of tricuspid valve are not normally located and positioned much below the true location. Sometimes, it can be seen as critical congenital heart defect in newborn period, in which neonates are very sick and may die if no active treatment started early.
Clinical Manifestations
In neonatal form with critical lesion, it generally presents in 48-72 hours of life when PDA is getting closed. It presents as a shock like state with dust dependent pulmonary situation. In early infancy, when disease is not in critical form, can presents in the form of bluish discoloration of lips and fingers etc. In childhood, it may be suspected on routine examination by asymptomatic murmur or ECG abnormalities.
For confirming the diagnosis, echocardiography is a definite modality.
Associated anomalies with Ebstein’s
Most commonly, it is associated with abnormalities of anterior leaflet of tricuspid vale, it can be enlargement, tethering of the leaflet.
About 70-80% cases, either a patent foramen ovale or atrial septal defect (ASD) between two upper chambers of heart is there.
In approx40-50% cases patient may have cardiac rhythm abnormalities in the form of either Wolff-Parkinson-White syndrome or heart blocks etc.
Management
Medical Treatment
Role of medication is in the management of cardiac rhythm disturbances that occurs frequently in Ebstein’s. In this setting, the preferred medication treatment agent is amiodarone. Since AV-blockade may promote conduction over the accessory pathway, drugs such as beta blockers, calcium channel blockers, and digoxin are contraindicated.
Surgery
Indications for surgery are:
- Critical and sick neonates
- Difficulty in doing routine activities with shortness of breath
- Cardiomegaly on chest X ray
- Bluish discoloration of lips and fingers
- Symptomatic severe valve regurgitation (TR)
- Stroke or brain related issues due to embolization in brain
Treatment of choice in Ebstein’s is surgical.
- Timing of surgery depends on age of presentation and severity of heart disease.
- In newborns who are dependent on the ductus (PDA) for its survival, either BT shunt or PDA stenting to be carries out as an emergency.
- In children, if surgical indication is there, then it can be in the form of repair of tricuspid valve, replacement of tricuspid valve if two ventricle repairs are possible. ASD needs to be closed simultaneously.
- Single ventricle palliation is the only option in the form of either PA band or BT shunt followed by Glenn shunt and then Fontan operation
- Please refer to double outlet ventricle in common cardiac condition for detailed information of these operations.