Interventional Pediatric Cardiology
Read More




Senior Consultant & In-charge
Interventional Pediatric Cardiology
Yatharth Super Speciality Hospital, Model Town, New Delhi
Saral Diagnostics, Pitampura, New Delhi
Formerly
Ex Senior Consultant at BLK MAX Super Speciality Hospital, Pusa Road, Delhi
Consultant in Pediatric Cardiology at Fortis Escorts Heart Institute and Research Centre, Okhla, New Delhi
Senior Registrar and Fellow in Pediatric Cardiology at Apollo Hospital, Hyderabad
The clinic provides comprehensive cardiac care for children with congenital and acquired heart conditions, from newborns through adolescents up to 18 years of age.
Diagnostic services include pediatric and fetal echocardiography, transesophageal echocardiography (TEE), ECG and Holter monitoring. Therapeutic offerings span a broad range of pediatric cardiac interventions as well as surgical management.
Dr. Agrawal works alongside a dedicated team of pediatric cardiac surgeons, intensivists and anaesthetists at Yatharth Super Speciality Hospital, Model Town — focusing on minimally invasive approaches wherever clinically appropriate and delivering compassionate, family-centred care.
His practice serves families from Delhi NCR and across India, and he regularly cares for international patients seeking specialist pediatric cardiology in Delhi.
Offering comprehensive diagnostics and treatment options

Patient Story — Successful ASD Closure

Patient Story — PDA Device Closure

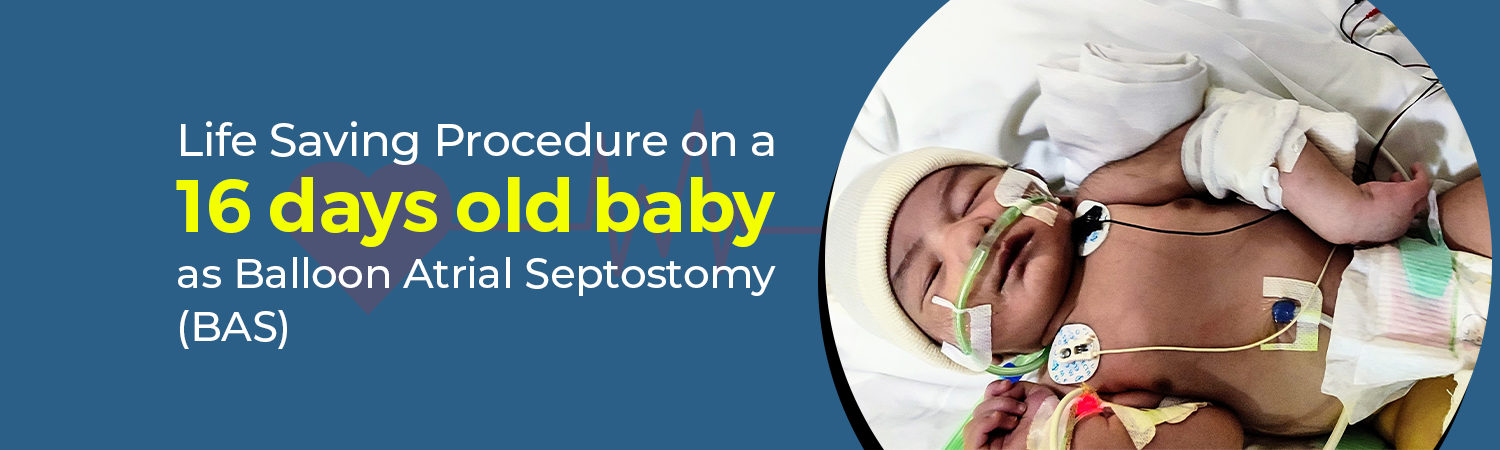
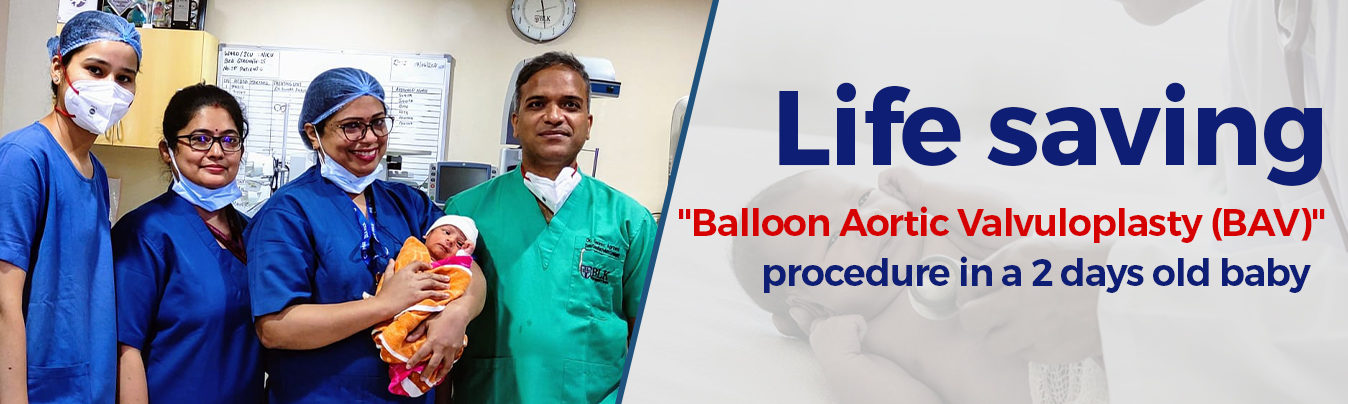
Patient Story — Balloon Valvuloplasty

Awareness — Congenital Heart Disease

Awareness — Pediatric Echocardiogram

Awareness — Fetal Echocardiogram
Real stories from families we have cared for
Dr. Agrawal explained our daughter's condition with great clarity. We left every consultation feeling reassured and informed about the next steps.
Excellent care from start to finish. The non-surgical device closure was successful and recovery was remarkably smooth for our son.
Calm, kind and highly skilled. Dr. Agrawal and his team made a stressful diagnosis feel manageable for our entire family.
Pediatric cardiology is the medical sub-speciality dedicated to diagnosing and treating heart conditions in fetuses, newborns, children and adolescents.
If a paediatrician suspects a heart murmur, irregular rhythm, breathlessness, bluish discolouration or poor growth, evaluation by a pediatric cardiologist is recommended.
Yes. Echocardiography uses sound waves only and is completely safe and painless — suitable even for premature newborns and unborn babies.
Many defects such as ASD, VSD and PDA can today be closed using catheter-based device closure as a minimally invasive alternative to open-heart surgery.