Newborns that have either pulmonary atresia or aortic atresia at birth are generally asymptomatic at the time of birth, but they need blood supply to either lung vessels or the body parts respectively hey are dependent upon patent ductus arteriosus (PDA) and PDA needs to be patent for survival of these newborns.
These newborns generally present in an emergency like situation if not detected on time. To keep these newborns alive, we need to do either surgery (known as modified BT shunt) or by a non-surgical technique known as Ductal Stenting or PDA stenting.
This is an alternative procedure to surgery (modified BT shunt) if surgery is considered to be a high risk or results of surgery may be suboptimal as compared to PDA stenting.
Indication of PDA stenting
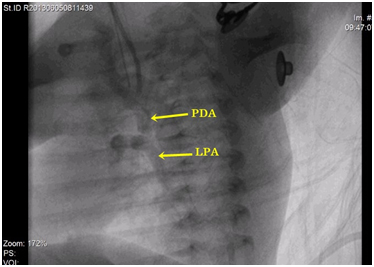
- Duct dependent pulmonary circulation: Cyanotic Newborns as seen in Pulmonary atresia like situations (seen in Tetralogy of Fallot (TOF), Ebstein’s anomaly, DORV, Tricuspid atresia etc) in which PDA is only source of blood supply to lung vessels is the most common indication.
- Duct dependent systemic circulation:Seen in Aortic atresia, Hypoplastic left heart syndrome (HLHS), critical aortic stenosis or coarctation of aorta. In all these conditions, neonatal survival depends of the patency of PDA.
By doing PDA stenting, blood supply to lungs or the body parts can be increased and this will keep the baby alive for next few months till the next stage of palliation of final treatment plan.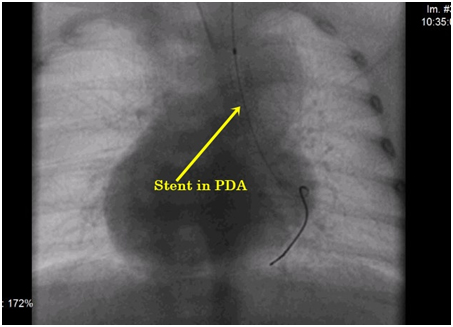
Procedural Details
Ductal Stenting is done angiographically in cath lab under fluoroscopy as a palliative procedure.
Procedure is done in general anesthesia in majority of the cases.
This procedure is done either from the femoral artery, axillary artery or carotid arterial accesses etc.
In this, we put a stent across the PDA so that size of closing PDA will increase for next few months.
After this procedure, we need to keep the baby in NICU for close monitoring as well as aspirin or other medications needs to be given for maintaining the patency of PDA.